
Introduction
- Only 0.5% to 2% of patients with a documented penicillin allergy who are given a penicillin will exhibit a hypersensitivity reaction, usually a rash or hives.
- True IgE-mediated penicillin allergies that cause anaphylaxis are rare.
- An IgE-mediated penicillin allergy can diminish over time — about 80% of patients become tolerant after a decade.
- Patients with a documented penicillin allergy may be inappropriately exposed to alternative antibiotics, resulting in increased treatment failures, adverse effects, and antimicrobial resistance.
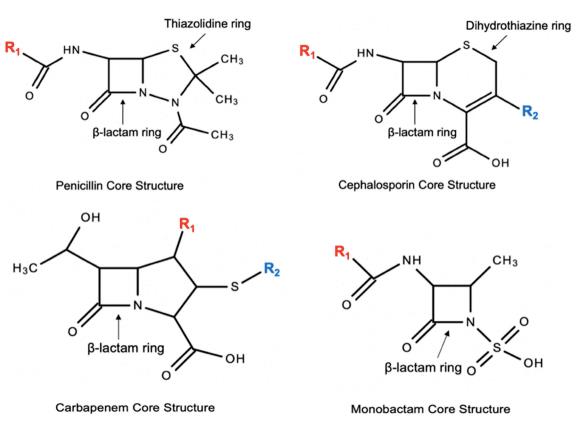
- Penicillins, cephalosporins, and carbapenems all share a beta-lactam core, raising the potential for cross-reactivity among these agents.
Pharmacology
- The drugs within each group below may cross-react with each other because they share similar side chains.
- Cross-reactivity between penicillins and cephalosporins is about 2%.
- Cefazolin is NOT likely to cross-react with penicillin (its side chain is not similar).
- Cross-reactivity with monobactams (e.g., aztreonam) is negligible.
- Cross-reactivity between penicillins and carbapenems is <1%.
| Group 1 | Group 2 | Group 3 | Group 4 |
|---|---|---|---|
| Penicillin Cefoxitin Cefuroxime | Amoxicillin Ampicillin Cefaclor Cephalexin Cefadroxil | Ceftriaxone Cefotaxime Cefuroxime Cefepime Cefpodoxime Ceftaroline | Aztreonam Ceftolozane Ceftazidime |
These groupings reflect structural side-chain similarity — a theoretical predictor of risk. Observed clinical cross-reactivity is low (~1–2%), and documented tolerance can override the chart: cefuroxime, for example, is listed here by side-chain similarity but was tolerated by all 244 challenged penicillin-allergic patients in Romano 2018. Agents in different groups do not share a side chain.
Evidence
| Author, year | Design | Intervention & comparison | Outcome |
|---|---|---|---|
| Mechanism — why cross-reactivity? | |||
| Nagakura, 1991 & Mayorga, 1995 | Animal / mechanistic studies | Antibodies formed when animals were immunized with protein–beta-lactam conjugates | 92% of antibodies recognized an epitope in which the side chain was the main constituent — the side chain is the most important determinant of penicillin immunogenicity |
| Cephalosporin cross-reactivity | |||
| Goodman, 2001 | Retrospective review (n = 2933) | Orthopedic patients with penicillin allergy receiving cefazolin before a procedure | Only 1 patient may have had a reaction — cefazolin cross-reactivity 0.33% |
| Daulat, 2004 | Retrospective review (n = 606) | Penicillin-allergic patients receiving cephalosporins (42% 1st-gen, 21% 2nd-gen, 37% 3rd/4th-gen) | Only 1 reaction (worsening eczema after cefazolin) — cross-reactivity 0.17% |
| Apter, 2006 | Retrospective review (n = 3920) | Penicillin prescription followed by a cephalosporin prescription; allergic-like events within 30 days | Cross-reactivity 1.1%; 70% had only urticaria; risk of anaphylaxis to cephalosporins only 0.001% |
| Romano, 2018 | Prospective study (n = 252) | IgE-mediated penicillin hypersensitivity: specific-IgE assays + skin tests to 10 cephalosporins; oral challenges if skin tests negative | 99 (39.3%) had positive cephalosporin tests, mostly to agents sharing side chains with penicillins; all 244 challenged tolerated cefuroxime axetil and ceftriaxone; 7 reacted to cefaclor or cefadroxil |
| Carbapenem cross-reactivity | |||
| Romano, 2006 | Prospective study (n = 112) | Penicillin skin-test-positive patients skin tested to imipenem; if negative, IM challenge | Only 1 positive imipenem skin test — cross-reactivity 0.9%; all 110 skin-test-negative patients tolerated the IM challenge |
| Romano, 2007 | Prospective study (n = 104) | Penicillin skin-test-positive patients skin tested to meropenem; if negative, IV challenge | Only 1 positive meropenem skin test — cross-reactivity 1%; all 103 skin-test-negative patients tolerated the IV challenge |
| Atanaskovic-Markovic, 2008 | Prospective study in children (n = 108) | Children with penicillin allergy skin tested to penicillin and meropenem; if negative, IV challenge | Only 1 positive meropenem skin test — cross-reactivity 0.9%; all 107 skin-test-negative children tolerated the IV challenge |
| Sánchez de Vicente, 2020 | Prospective study (n = 137) | Tolerance testing for cephalosporins and carbapenems in patients with confirmed penicillin allergy | 0/46 positive imipenem skin tests; 0.79% (1/137) positive to cefuroxime; 0.79% (1/137) positive to ceftriaxone |
| Recent evidence (2020–2026) — risk-stratification & de-labeling | |||
| Trubiano, 2020 (PEN-FAST) | Derivation & validation cohort (n = 460 in validation) | Clinical decision rule to risk-stratify reported penicillin allergy | A PEN-FAST score <3 = low risk; only 3.7% of low-risk patients had a positive test (negative predictive value 96.3%) — supports challenge without prior skin testing |
| Copaescu, 2023 (PALACE) | Randomized noninferiority trial (n = 377) | Direct oral amoxicillin challenge vs. skin testing followed by oral challenge in low-risk penicillin allergy | Positive reactions 0.5% (1/187) with direct oral challenge vs. 0.5% (1/190) with skin-test-first — direct oral challenge was noninferior |
| Khan, 2022 (Practice Parameter) | AAAAI / ACAAI / JCAAI guideline | 2022 Drug Allergy Practice Parameter update | Supports direct oral amoxicillin challenge without prior skin testing in selected low-risk patients (e.g., distant benign cutaneous reactions) — a key de-labeling recommendation |
Conclusions
- True penicillin allergies are less common than reported, and anaphylaxis is uncommon.
- Cross-reactivity among penicillins and cephalosporins is attributed to similarity in side chains.
- Cephalosporin cross-reactivity with penicillins is much lower than reported in early studies, partly because of contamination of the older study drugs with penicillin.
- Cross-reactivity between penicillins and cephalosporins is about 2%, and with carbapenems is <1%.
- These cross-reactivity rates have not materially changed; what has shifted is practice toward penicillin-allergy de-labeling. Validated risk-stratification (PEN-FAST, 2020) identifies low-risk patients in whom direct oral amoxicillin challenge without prior skin testing is safe (PALACE RCT 2023; 2022 Drug Allergy Practice Parameter).
- For low-risk patients, de-labeling often makes cross-reactivity calculations unnecessary. When a true penicillin allergy is confirmed, selecting a cephalosporin or carbapenem with a dissimilar side chain (e.g., cefazolin) keeps cross-reactivity low.
References
- Apter AJ, Kinman JL, Bilker WB, et al. Is There Cross-Reactivity Between Penicillins and Cephalosporins? Am J Med. 2006;119(4):354e11-19.
- Atanaskovic-Markovic M, Gaeta F, Medjo B, Viola M, Nestorovic B, Romano A. Tolerability of Meropenem in Children with IgE-Mediated Hypersensitivity to Penicillins. Allergy. 2008;63:237-240.
- Blumenthal KG, Shenoy ES, Wolfson AR, et al. Addressing Inpatient Beta-Lactam Allergies: A Multihospital Implementation. J Allergy Clin Immunol Pract. 2017;5(3):616-625.
- Blumenthal KG, Huebner EM, Fu X, et al. Risk-Based Pathway for Outpatient Penicillin Allergy Evaluations. J Allergy Clin Immunol Pract. 2019;7(7):2411-2414.
- Campagna JD, Bond MC, Schabelman E, Hayes BD. The Use of Cephalosporins in Penicillin-Allergic Patients: A Literature Review. J Emerg Med. 2012;42(5):612-620.
- Chaudry SB, Veve MP, Wagner JL. Cephalosporins: A Focus on Side Chains and Beta-Lactam Cross-Reactivity. Pharmacy. 2019;7:1-16.
- Daulat S, Solensky R, Earl HS, Casey W, Gruchalla RS. Safety of Cephalosporin Administration to Patients with Histories of Penicillin Allergy. J Allergy Clin Immunol. 2004;113(6):1220-1222. doi: 10.1016/j.jaci.2004.03.023.
- DePestel DD, Benninger MS, Danziger L, et al. Cephalosporin Use in Treatment of Patients with Penicillin Allergies. J Am Pharm Assoc. 2008;48:530-540.
- Goodman EJ, Morgan MJ, Johnson PA, Nichols BA, Denk N, Gold BB. Cephalosporins can be Given to Penicillin-Allergic Patients Who Do Not Exhibit an Anaphylactic Response. J Clin Anesth. 2001;13(8):561-564.
- Mayorga C, Obispo T, Jimeno L, et al. Epitope Mapping of Beta-Lactam Antibiotics with the Use of Monoclonal Antibodies. Toxicology. 1995;97:225-234.
- Nagakura N, Souma S, Shimizu T, Yanagihara Y. Anti-Ampicillin Monoclonal Antibodies and their Cross- Reactivities to Various Beta-Lactams. J Antimicrob Chemother. 1991;28(3):357-368. doi: 10.1093/jac/28.3.357.
- Romano A, Viola M, Gueant-Rodriguez RM, Gaeta F, Pettinato R, Gueant JL. Imipenem in Patients with Immediate Hypersensitivity to Penicillins. N Engl J Med. 2006;354:2835-2837.
- Romano A, Viola M, Gueant-Rodriguez RM, Gaeta F, Valluzzi R, Gueant JL. Brief Communication: Tolerability of Meropenem in Patients with IgE-Mediated Hypersensitivity to Penicillins. Ann Intern Med. 2007;146:266-269.
- Shenoy ES, Macy E, Rowe T, Blumenthal KG. Evaluation and Management of Penicillin Allergy: A Review. JAMA. 2019;321(2):188-199.
- Sánchez de Vicente J, Gamboa P, García-Lirio E, Irazabal B, Jáuregui I, Martínez MD, Segurola A, Seras Y, Galán C. Tolerance to Cephalosporins and Carbapenems in Penicillin-Allergic Patients. J Investig Allergol Clin Immunol. 2020;30(1):75-76. doi: 10.18176/jiaci.0463. Epub 2019 Nov 4. PMID: 31680067.
- Romano A, Valluzzi RL, Caruso C, Maggioletti M, Quaratino D, Gaeta F. Cross-Reactivity and Tolerability of Cephalosporins in Patients with IgE-Mediated Hypersensitivity to Penicillins. J Allergy Clin Immunol Pract. 2018 Sep-Oct;6(5):1662-1672. doi: 10.1016/j.jaip.2018.01.020. Epub 2018 Feb 3. PMID: 29408440.
- Khan DA, Banerji A, Blumenthal KG, et al. Drug allergy: A 2022 practice parameter update. J Allergy Clin Immunol. 2022;150(6):1333-1393. doi: 10.1016/j.jaci.2022.08.028.
- Trubiano JA, Vogrin S, Chua KYL, et al. Development and Validation of a Penicillin Allergy Clinical Decision Rule. JAMA Intern Med. 2020;180(5):745-752. doi: 10.1001/jamainternmed.2020.0403.
- Copaescu AM, Vogrin S, James F, et al. Efficacy of a Clinical Decision Rule to Enable Direct Oral Challenge in Patients With Low-Risk Penicillin Allergy: The PALACE Randomized Clinical Trial. JAMA Intern Med. 2023;183(9):944-952. doi: 10.1001/jamainternmed.2023.2986.
Tags:penicillin allergy
cross-reactivity
cephalosporin
carbapenem
Never Miss a Friday Pearl
Get Pharmacy Pearls in your inbox every Friday
Free weekly clinical pearls written for pharmacists. Practical, evidence-based, and built for bedside use.
Free forever. Unsubscribe anytime. No spam, ever.