Pharmacology
- Mechanism of Action: Anti-dopaminergic (D2 receptor antagonist)
- 1st Generation Antipsychotic in the same class as haloperidol,
- Histamine and serotonin antagonist properties.
Droperidol was also widely used for the treatment of many other conditions: headache, nausea, agitation, and acute and chronic pain.

- Route of Administration: Both the IV and IM administration routes have been shown effective
- Dose: The most commonly used dose being 5 mg and the maximum total dose being 10 mg.
- Onset – 15-30 min
- First-line Agent: Droperidol can be used as a first-line agent for agitation, alone or in combination with midazolam.
Adverse Effects:
- There is a risk of extrapyramidal effects: dystonia, akathisia, and pseudoparkinsonism
- These adverse effects are usually brief, dose related, and can be treated with a histamine blocker like diphenhydramine (25-50 mg IV) or benztropine
- Neuroleptic malignant syndrome (NMS) has been seen with use of droperidol, as with other antipsychotics
- Potential for hypotension and oversedation
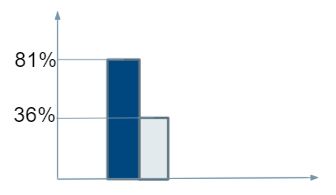
Efficacy
Small, double-blind clinical trial involving 27 patients, droperidol 5 mg IM was compared to haloperidol 5 mg IM Droperidol additional sedatives)
- At 30 minutes, 81% of the haloperidol-treated patients needed additional sedatives compared to 36% of the droperidol-treated patients
| Study | Design | Outcome |
| Hill CH, Miner JR, Martel ML. Olanzapine versus droperidol for the treatment of primary headache in the emergency department. Acad Emerg Med. 2008;15:806-811) | The effects of droperidol 5 mg IV and olanzapine 5 mg IV in adult ED patients requiring pharmacologic sedation for acute agitation in a randomized, double-blind, placebo-controlled fashion with incremental IV midazolam boluses until adequate sedation was achieved. | IV droperidol used as an adjunct to midazolam is effective and decreases time to adequate sedation when compared with midazolam monotherapy (mean, 21.3 minutes vs 67.8 minutes) |
| Cole JB, Klein LR, Martel ML. Parenteral antipsychotic choice and its association with emergency department length of stay for acute agitation secondary to alcohol intoxication. Acad Emerg Med. 2019;26:79-84. | Parenteral antipsychotic use for agitation was evaluated in a study of agitated patients intoxicated on alcohol who received a single parenteral dose of an antipsychotic: droperidol (n = 3,790), haloperidol (n = 1,449) or olanzapine (n = 6,548) | Patients who received droperidol had a shorter median ED length of stay (499 minutes; 95% CI, 493-506 minutes) than those who received haloperidol (524 minutes; 95% CI, 515-537 minutes) or olanzapine (533 minutes; 95% CI, 528-539 minutes). |
| Taylor DM, Yap CYL, Knott JC. Midazolam-Droperidol, Droperidol, or Olanzapine for Acute Agitation: A Randomized Clinical Trial. Ann Emerg Med. 2017 Mar;69(3):318-326.e1. | The effects of droperidol 5 mg IV+ Midazolam, droperidol IV 5 mg monotherapy, and olanzapine 5 mg IV in adult ED patients requiring pharmacologic sedation for acute agitation in a randomized, double-blind, placebo-controlled fashion | Ten minutes after the first dose, significantly more patients in the midazolam-droperidol group were adequately sedated compared with the droperidol and olanzapine groups. Patients in the midazolam-droperidol group required fewer additional doses or alternative drugs to achieve adequate sedation. The 3 groups’ adverse event rates and lengths of stay did not differ. |
Controversy
- Withdrawn from market for QTc prolongation and Sudden Death
- “Red flags went up across the medical community resulting in a number of admirable independent reviews of the FDA data from which this warning was based upon (19, 22-24)
- Jackson CW, Sheehan AH, Reddan JG. Evidence-based review of the black-box warning for droperidol. Am J Health Syst Pharm. 2007;64:1174-86.
- Horowitz BZ, Bizovi K, Moreno R. Droperidol–behind the black box warning. Acad Emerg Med. 2002;9:615-8.
- Kao LW, Kirk MA, Evers SJ, Rosenfeld SH. Droperidol, QT prolongation, and sudden death: what is the evidence? Ann Emerg Med. 2003;41:546-58.
- Newman DH. Training the Mind, and the Food and Drug Administration, on Droperidol. Ann Emerg Med. 2015;66:243-5.
- “One such review pointed out that 83% of the cases of QT prolongation were received from nations outside the United States with 49% of fatalities from droperidol occurring at doses of 50 mg or greater (up to 150mg)– multitudes higher than our typical dosing of 5 to 10 mg (25). Additionally, of the 273 cases that made up the black box warning, only 94 were unique cases identified as ‘associated’ with droperidol use (the rest duplicates)”
- van Zwieten K, Mullins ME, Jang T. Droperidol and the black box warning. Ann Emerg Med. 2004;43:139-40.
- “Red flags went up across the medical community resulting in a number of admirable independent reviews of the FDA data from which this warning was based upon (19, 22-24)
Cole et al 2020 Safety Data
| Background | Objectives | Patient population | Intervention/ Comparison | Outcomes |
| Droperidol carries a boxed warning from the US FDA for QT prolongation and TdP in 2001 . After a six-year hiatus, droperidol again became widely available in the US in early 2019. With its return, clinicians must again make decisions regarding the boxed warning | To report the incidence of QT prolongation or TdP in patients receiving droperidol in the ED | Patients receiving droperidol at an urban Level I trauma center from 1997–2001 were identified via electronic health record query | Reviewed electrocardiogram (ECG) data for both critically-ill and noncritical patients and recorded Bazett’s corrected QT intervals (QTc). ECGs from critically-ill patients undergoing resuscitation were further riskstratified using the QT nomogram | The incidence of QTc prolongation and TdP in ED patients receiving droperidol to be extremely rare. Data suggest the FDA “black box warning” is overstated, and that close ECG monitoring is useful only in high-risk patients |
Calver et al 2020 Safety Data
| Objectives | Design | Outcomes |
| To investigate the frequency ofQT prolongation and torsades de pointes in patientsadministered high-dose (10 mg or more) droperidol in theED for acute behavioral disturbance. | Patients receiving droperidol at in 6 EDs requiring parenteral sedation for acute behavioral disturbance with ECG within 2 hours of drug administration. | The incidence of QTc prolongation was 13 of the 1,009 patients (1.3%; 95% confidence interval 0.7% to 2.3%), but 7 of these had another cause attributed for prolonged QT . Adverse events occurred in 70 patients (5%) and oversedation without complications in 109 (8%), the latter more common for patients receiving benzodiazepines as additional sedation (16/109 [15%]) |
When we should use Droperidol
When Not to Use Droperidol