Participants 427





– Treat underlying condition
– Support oxygenation and ventilation
– Consider pharmacotherapy
– Rescue options for refractory hypoxemia
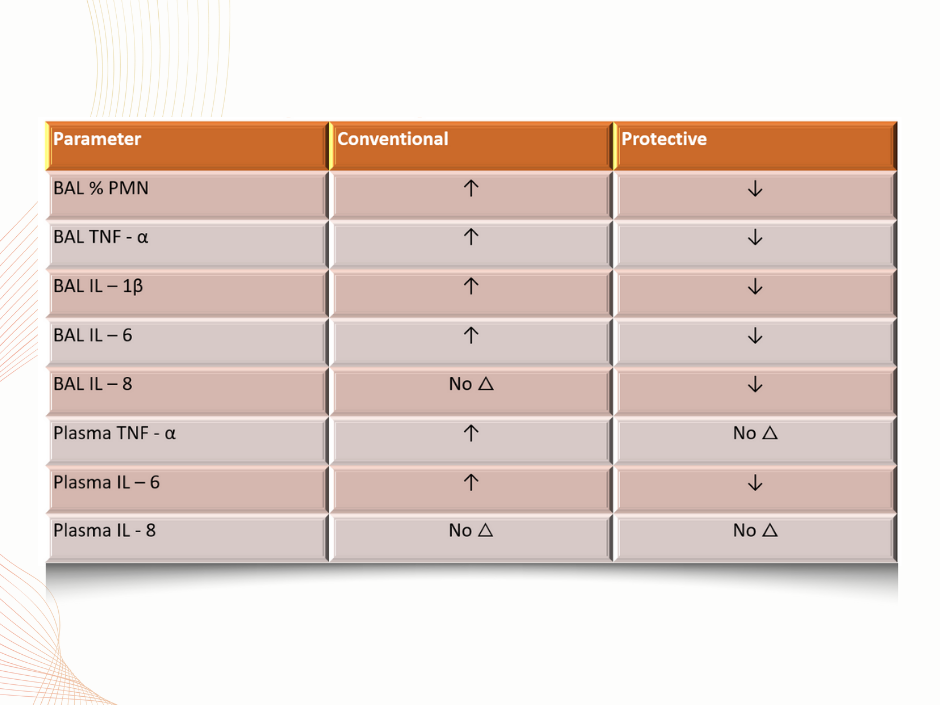
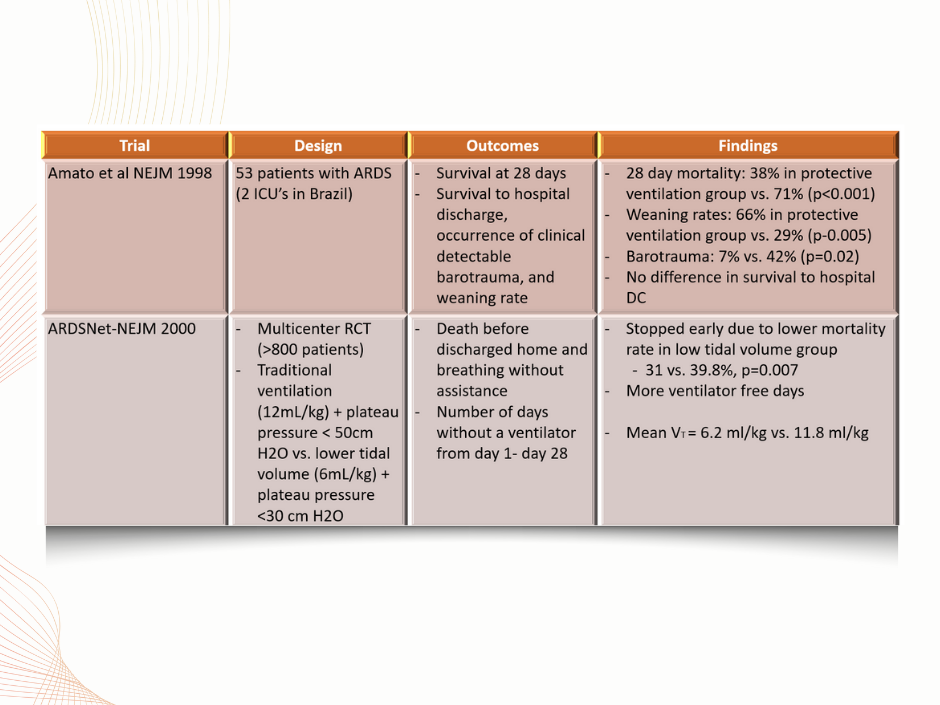
- A lung-protective ventilatory strategy is advocated to reduce lung injury.
- The ARDS Clinical Network Mechanical Ventilation Protocol (ARDSnet) sets the following goals:
- Tidal volume (V) from 4 to 8 mL/kg of ideal body weight (IBW)
- Respiratory rate (RR) up to 35 bpm
- SpO2 88% to 95%
- Plateau pressure (P) less than 30 cm H2O
- pH goal 7.30 to 7.45, and inspiratory-to-expiratory time ratio less than 1.
- High tidal volumes may promote further lung injury:
- Volutrauma
- Barotrauma
- Guideline Recommendation: We recommend limiting tidal volume to 4–8 mL/kg for mechanically ventilated adult patients with ARDS (GRADE 1D).
Mechanical Ventilation
Treatment
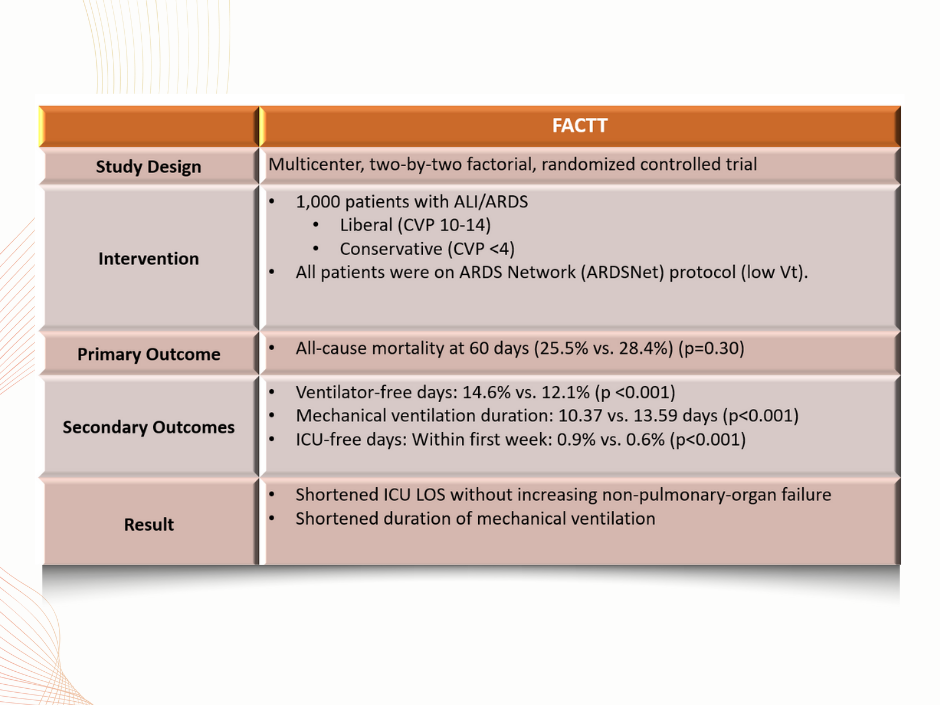
- Increased lung edema is present due to capillary leak
- Impairs oxygen diffusion at alveolar level
- Goal: Reduce extra-vascular lung edema and reduce preload filling pressures
- Guideline Recommendation: We suggest performing the restrictive fuid management strategies for adult patients with ARDS (weak recommendation/moderate certainty of evidence: GRADE 2B).
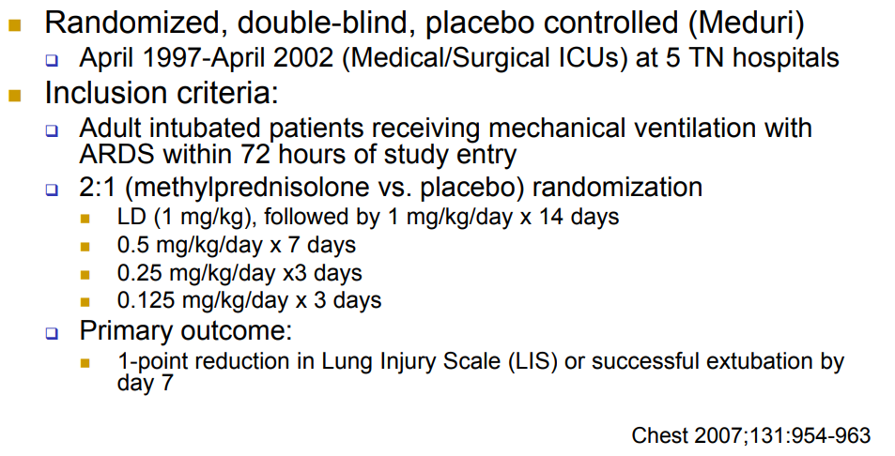
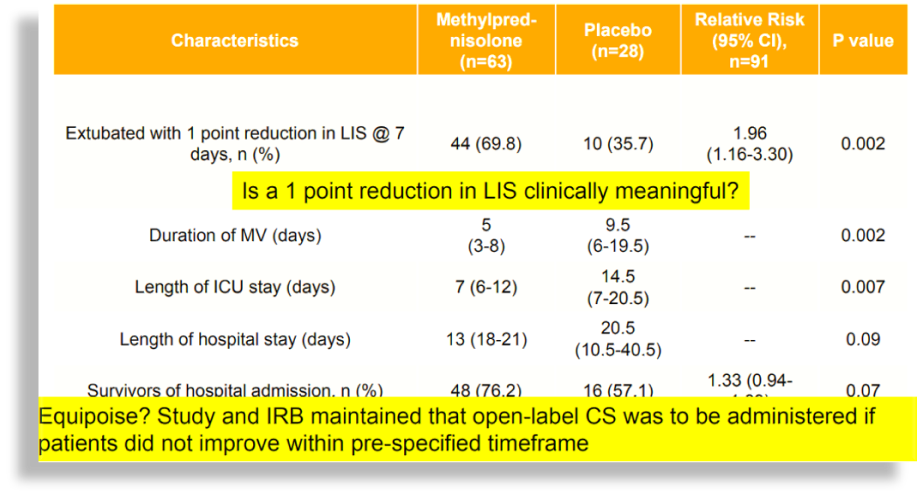
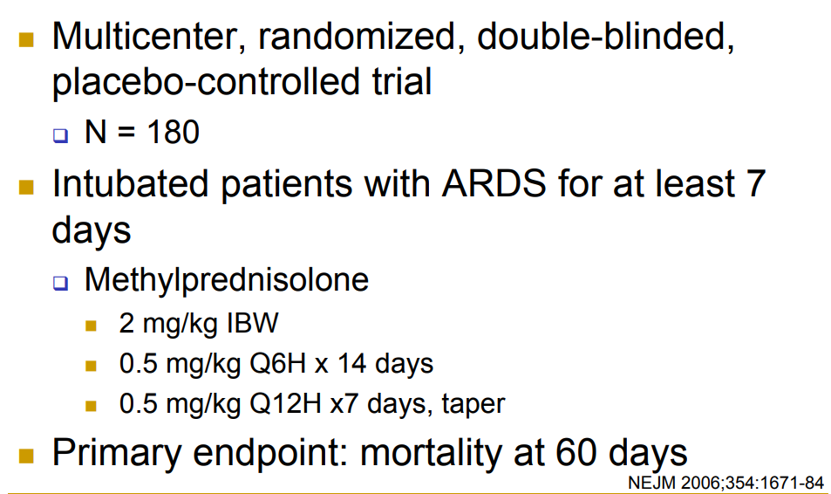
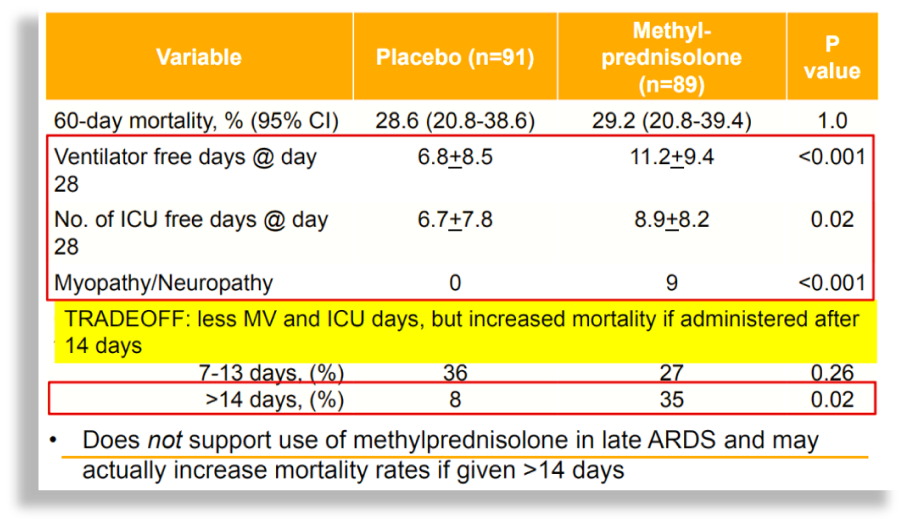
- The pathogenesis of ARDS is a permeability pulmonary edema due to nonspecific inflammation, and whether anti-inflammatory corticosteroids improve clinical outcomes is an important clinical question.
- Investigated in:
- Early ARDS (< 72 hours)
- Late ARDS ( > 7 days)
- Guideline Recommendation:
- We suggest against using high-dose corticosteroids for adult patients with ARDS. (GRADE 2C).
- We recommend using low-dose corticosteroids for adult patients with ARDS. (GRADE 1B).
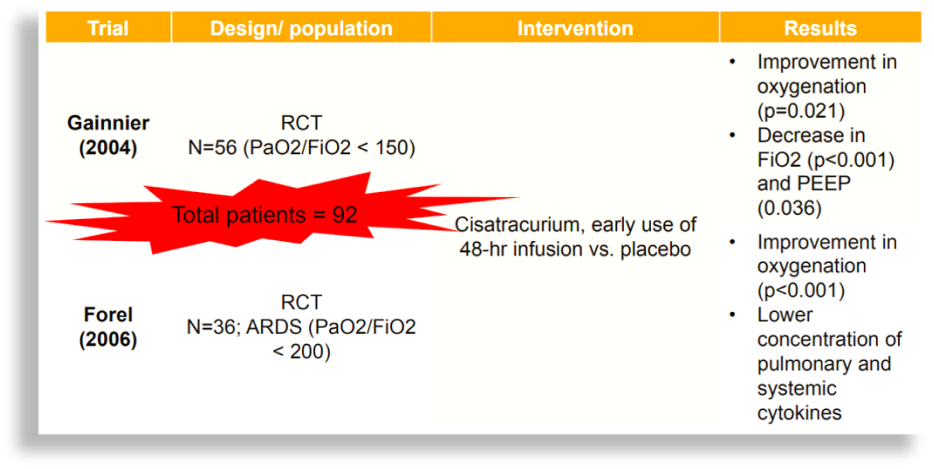
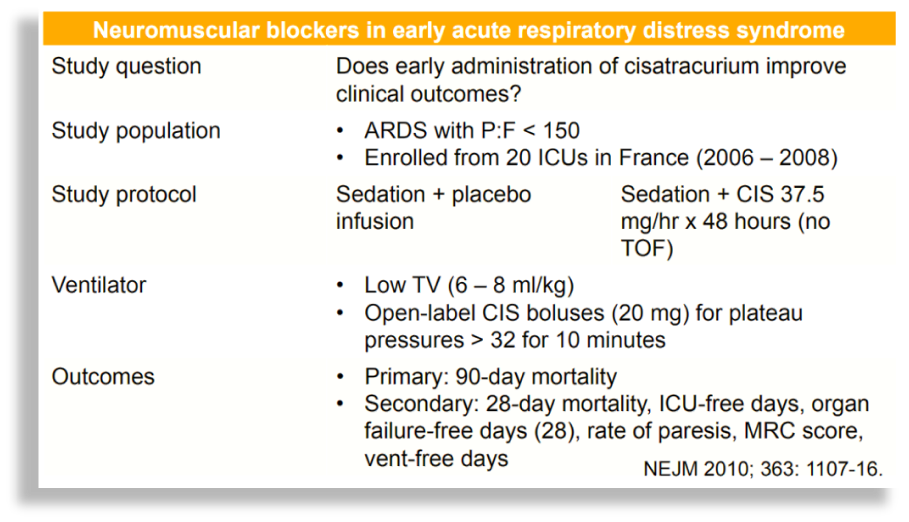
- Muscular paralysis induced by NMBA will prevent spontaneous respiratory movements, reducing desynchrony and improving gas exchange
- Additional benefits include increasing chest wall compliance and improve MV during ARDS
- Allows for better adaptation to protective ventilation strategy
- Reduction in pulmonary inflammation possibly leading to improvement in oxygenation
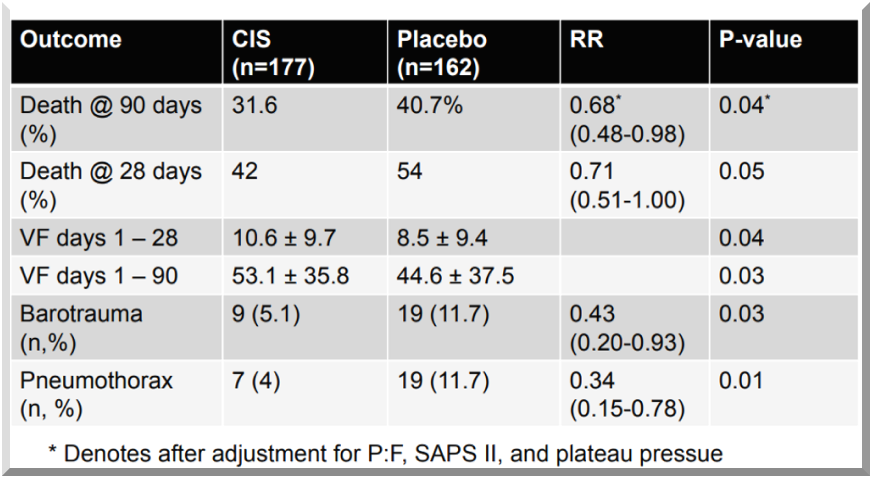
- Guideline Recommendation:
- We suggest administering neuromuscular blockers at an early phase for adult patients with moderate or severe ARDS (GRADE 2D).
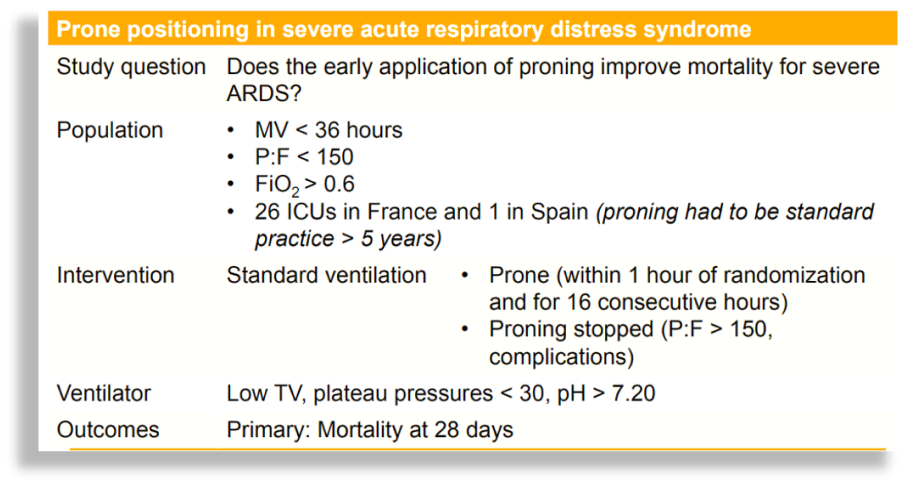
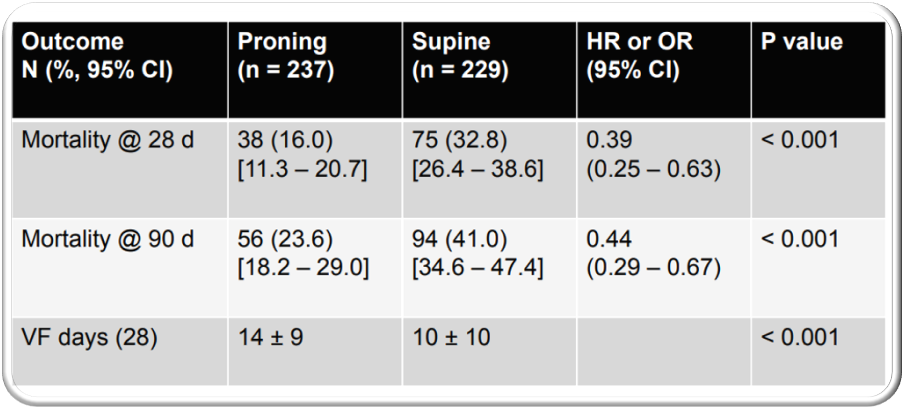
- Proning: Patient turned to face down
- Theoretical Benefit:
- May also allow the abdomen to expand more and facilitate better movement of diaphragm
- Facilitate drainage of pulmonary secretions
- Eliminate compression of lungs by the heart
- Guideline Recommendation: We suggest performing the prone positioning in adult patients with moderate or severe ARDS for long periods of time (GRADE 2D).