
Electrocardiogram
- Diagnosis of hyperkalemia starts with identifying if the increase in serum K+ levels is caused by pseudohyperkalemia. If it is, no further action required. If not, assess the serum K+ level and check for ECG changes. If K+ is ≥ 6.0 and ECG changes are present, recommend for emergency therapy.
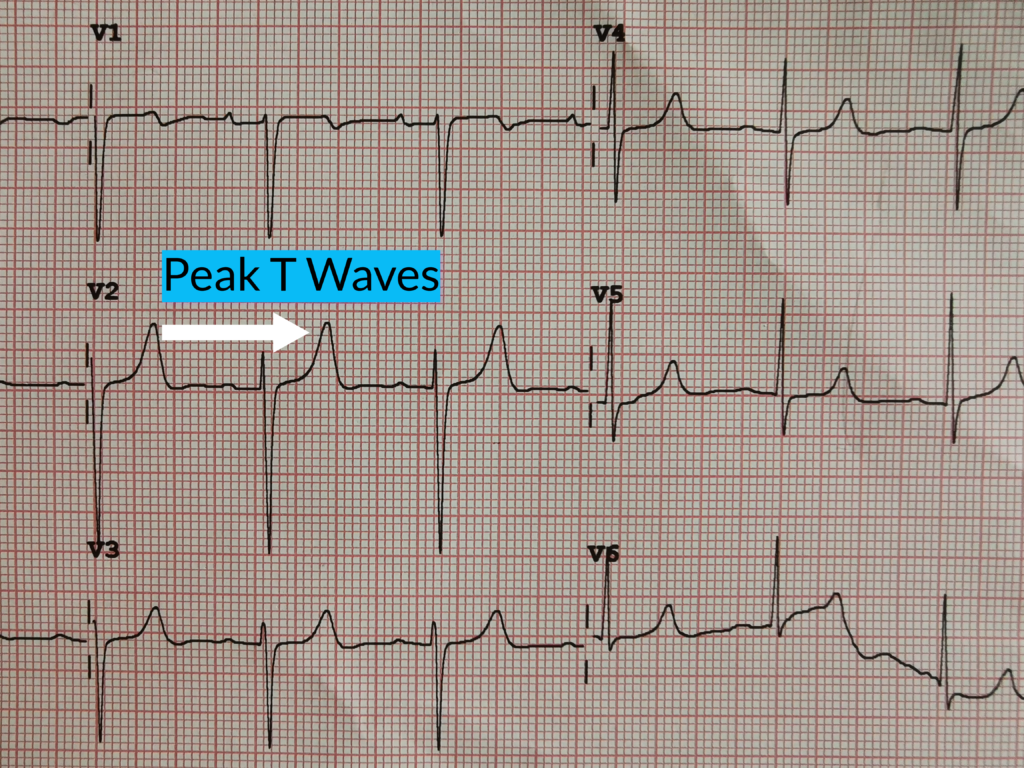
An ECG alone is unreliable in the certainty of hyperkalemia. But, there are potential ECg changes that may predict serum K+ levels.
| Serum Potassium | Potential ECG Changes |
| Mild Hyperkalemia 5.5 – 6.5 mEq/L | Tall, peaked T waves with narrow base QT Interval shortening ST-segment depression |
| Moderate Hyperkalemia 6.5 – 8.0 mEq/L | Peaked T waves PR-interval prolongation P wave decreased amplitude or disappearance QRS widening R-wave amplification |
| Severe Hyperkalemia> 8.0 mEq/L | P-wave absence QRS widening Intraventricular/fascicular/bundle branch blocks Sine wave |
Accuracy in diagnosis is coupled with intensive history taking to identify dietary factors that may be associated with increased potassium load, physical examination to check for the patient’s general state of health, as well as basic laboratory tests for confirmatory on the K+ serum levels.
Confirmatory testing
- A repeat laboratory testing to confirm for pseudohyperkalemia must be carried out before proceeding with treatment. This is especially in the absence of any predisposing factors that suggest hyperkalemia such as dietary factors or medications and in patients without kidney disease.
- Once pseudohyperkalemia is ruled out, initial treatment depends on the severity of the signs and symptoms as well as the severity of the K+ serum level elevation. In all patients, underlying cause for increased potassium load should be eliminated.