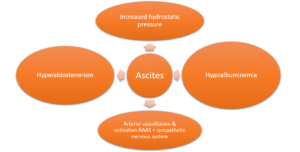
Pathophysiology
Evaluation
- Paracentesis
- Serum albumin ascites gradient (SAAG)
- SAAG = Albuminserum – Albuminascitic fluid
- SAAG ≥ 1.1g/dL implies portal hypertension is present
Ascites Treatment
| 1ST LINE | |
| Alcohol Cessation | Treat underlying cause |
| Sodium Restriction | 2000 mg per day |
| Diuretics | Spironolactone & Furosemide:
•Ratio of 100:40 •Max Dose: 400 mg spironolactone, 160 mg furosemide |
| 2ND LINE | |
| Paracentesis | Albumin:
•≤ 5 L – None •> 5 L – 6 to 8 g per liter removed |
| BP Medication Adjustments | Discontinuation of ACE-I, ARB, BB
•MAP > 82 mmHg |
| Midodrine | Add to diuretics in hypotensive patients:
•Dosing: 7.5 mg TID |
| Refractory | |
| Serial Therapeutic Paracentesis, TIPS, Peritoneovenous Shunts, Transplant | |
| Agent | Dose | MOA | Onset of Effect | Dose Limiting Effects |
| Spironolactone | Initial: 12.5-100 mg
Max: 400 mg |
– Aldosterone antagonist
– Decreases aldosterone effect in distal tubules |
3-5 days | -Gynecomastia
-Hyperkalemia |
| Furosemide | Initial: 40 mg
Max: 160 mg |
-Loop diuretic
-Blocks reabsorption of Na+ in Loop of Henle, ↑ Mg 2+ and Ca 2+ excretion |
3-5 days | -Hypotension
-Intravascular dehydration |