
-
Background
Introduction -
Pathophysiology & Diagnostics
-
Emergent TherapyBenzodiazepines For Status Epilepticus
-
What Agents to Use When No IV Access with Kyle Hultz
-
Clinical Trials for the Use of Benzodiazepines in SE
-
Summary of The Use of Benzodiazepines for Emergent Therapy of SE
-
Urgent TherapyWhat's Your Agent of Choice After Benzodiazepines in Status Epilepticus with Kyle Hultz
-
Anti-Epileptic Drugs (AED) in SE
-
Clinical Trials for the Use of Anti-Epileptic Drugs in SE
-
Refractory Status EpilepticusPharmacologic Agents For Refractory Status Epilepticus
-
Clinical Trials for the Use of Drugs in RSE
-
ConclusionSummary & References
-
The Decision to Intubate a Patient in Status Epilepticus with Richard Tsen
Participants 426





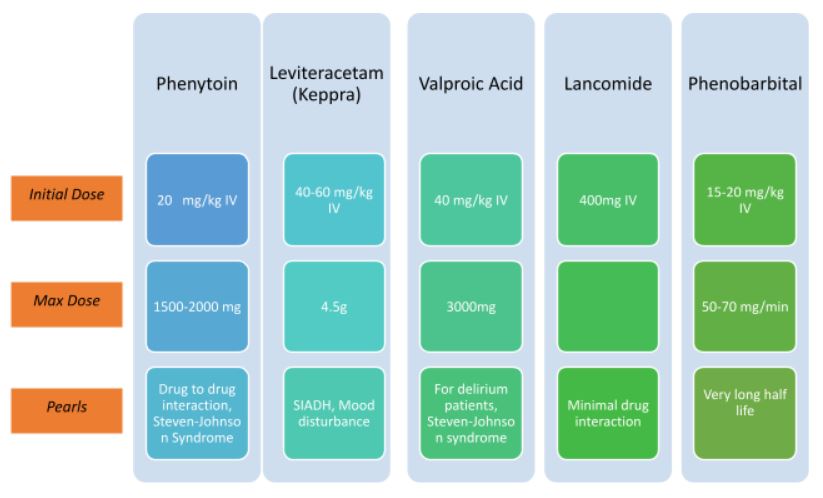

Use of Anti-epileptic Drugs (AED) in SE
For patients with continuous seizure activity despite the use of emergency Benzodiazepine therapy, Anti-epileptic Drugs (AED) must be added. These drugs include Phenytoin, Levetiracetam, Valproic Acid, Lacosamide, and Phenobarbital all given intravenously. These drugs do not have a significant benefits over the others.
These anti-epileptic drugs are used following the initial dose of Benzodiazepine to further manage continuous seizures. This is considered the second therapy phase and is done when the seizure persists at the 20-minute mark.
1. Phenytoin or Fosphenytoin
- Mechanism of Action: Blockade of voltage-dependent membrane sodium channels that increases action potential therefore obstructing positive feedback that sustains repetitive seizures
- Route of Administration: Intravenous
- Dose:
- Phenytoin: 20 mg/kg IV, maximum infusion rate: 50 mg/min
- Fosphenytoin: 20 mg/kg PE IV, maximum infusion rate: 150 mg/min, may add 5-10 mg/kg for persistent seizures
- Maintenance Dose: 5-7 PE/kg/day in 2-3 divided doses
- PE = Phenytoin Equivalent
- Pharmacokinetics: Absorbed entirely at 1.5 to 3 hours, but absorption may last logner than 2 weeks due to reduction of effects of GI motility and poor water solubility
- Adverse Effects: Hypotension, bradycardia, Steven-Johnsons syndrome, Pancytopenia, Delirium
- Comments or Pearls: Avoid combination with Valproate, Numerous contraindications (pregnancy, hepatic and renal dysfunction) and adverse effects thus is not the first agent for second-line therapy of SE
2. Levetiracetam (Keppra)
- Mechanism of Action: Involves neuronal binding to synaptic vesicle protein, inhibiting calcium release therefore opposing the activity of negative modulators of GABA
- Route of Administration: Intravenous
- Dose: 20-60 mg/kg IV, maximum infusion rate of 4.5g over 10 minutes
- Maintenance Dose: 1 – 1.5g q12hr
- Pharmacokinetics: Infuses rapidly, with same equivalent efficacy as that of Fosphenytoin and Valproate for SE
- Adverse Effects: Syndrome of Inappropriate AdH (SIADH), Mood Disturbance
- Comments or Pearls: Generally the preferred AED as second-line therapy for SE because of zero contraindications, Avoid combination with Fosphenytoin, Renally cleared therefore maintenance dose need not be adjusted based on renal function
3. Valproic Acid
- Mechanism of Action: acts on GABA levels in the CNS and blocks voltage-gated ion channels to prevent further seizure propagation
- Route of Administration: Intravenous
- Dose: 40 mg/kg IV, maximum infusion rate up to 3000mg over 5-10 minutes, may add 20 mg/kg over 5 minutes
- Maintenance Dose: 30-60 mg/kg daily, divided TID
- Pharmacokinetics: 13 – 19 hours halflife
- Adverse Effects: Hyperammonemia, Encepalopathy, Steven-Johnson syndrome, SIADH, Pancreatitis, Hepatotoxicity, Thrombocytopenia
- Comments or Pearls: Used for mood stabilization therefore is a good choice for patients with agitated delirium or known psychiatric disorders; Interferes with pharmacokinetics of Phenytoin and Phenytoin equivalents and Phenobarbital; Contraindicated to pregnant patients
4. Lacosamide (Vimpat)
- Mechanism of Action: Inhibits voltage-gated sodium channels
- Route of Administration: Intravenous
- Dose: 400mg IV over 5 minutes
- Maintenance Dose: 200 mg IV q12hr
- Pharmacokinetics: Minimally bound to plasma protein with no known relevant drug to drug interactions, half-life of 14 hours
- Adverse Effects: Atrioventricular block, Hypotension
- Comments or Pearls: New agent with safe and minimal drug interactions
5. Phenobarbital
- Mechanism of Action: acts on GABA receptors to increase synaptic inhibition
- Route of Administration: Intravenous
- Dose: 15-20 mg/kg IV, maximum infusion rate of 50-70 mg/min
- Pharmacokinetics: Long half-life increases risk of prolonged sedation
- Adverse Effects: Somnolence, Respiratory Suppression
- Comments or Pearls: Preferred anti-epileptic for alcohol withdrawal seizures, useful to assist in weaning patients off a barbiturate coma
